Publications
Dr. Christos talking on ANT1 about periodontal disease and systemic health with Nikitas Kyriakou
{kind=link}
MicroRNAs regulate cytokine responses in Gingival Epithelial Cells
MicroRNAs (miRNAs) have been established as key regulators of various biological processes with possible involvement in the pathobiology of periodontal disease. Expanding our earlier observations of substantial differential expression of specific miRNAs between clinically healthy and periodontitis-affected gingival tissues, we used miRNA inhibitors (sponges) in loss-of-function experiments to investigate the involvement of specific miRNAs in the response of pocket epithelium-derived, telomerase-immortalized human gingival keratinocytes (TIGKs) to microbial infection. We constructed stable knockdown (KD) cell lines for five epithelium-expressed miRNAs (miR-126, miR-141, miR-155, miR-210, and miR-1246) and assessed their response to infection with periodontal pathogens using microarray analysis, quantitative PCR (qPCR), enzyme-linked immunosorbent assay (ELISA), and Western blot assay.
*Reference: Chen SC, Constantinides C, Kebschull M, Papapanou PN. MicroRNAs regulate cytokine responses in gingival epithelial cells. Infection and immunity. 2016 Dec 1;84(12):3282-9.
{kind=link}
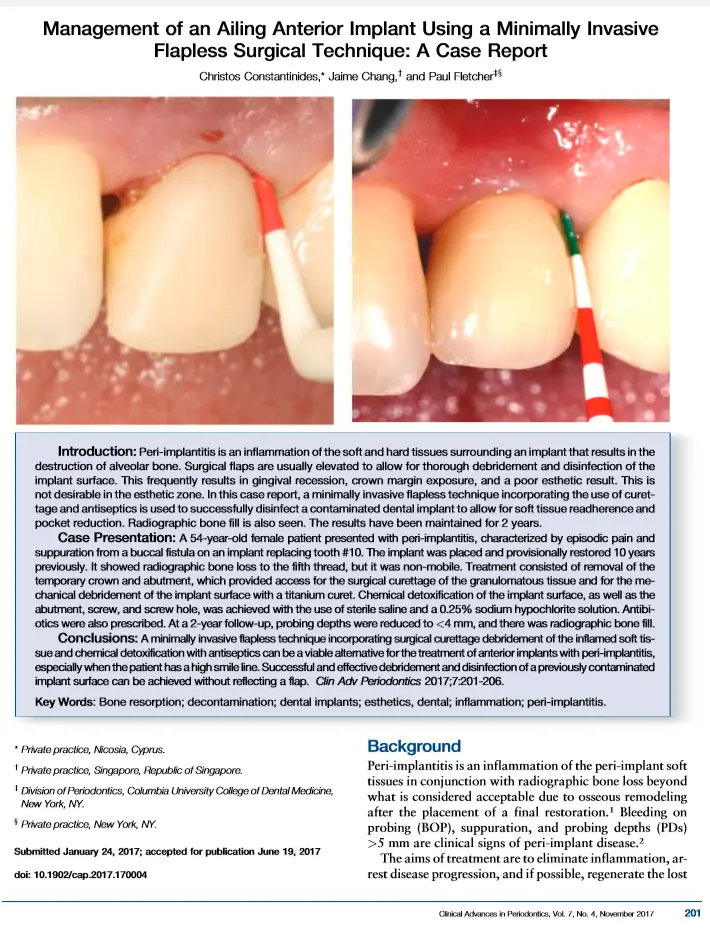
Management of an ailing anterior implant using minimally invasive flapless surgical technique: A case report
Peri-implantitis is an inflammation of the soft and hard tissues surrounding an implant that results in the destruction of alveolar bone. Surgical flaps are usually elevated to allow for thorough debridement and disinfection of the implant surface. This frequently results in gingival recession, crown margin exposure, and a poor esthetic result. This is not desirable in the esthetic zone. In this case report, a minimally invasive flapless technique incorporating the use of curettage and antiseptics is used to successfully disinfect a contaminated dental implant to allow for soft tissue readherence and pocket reduction. Radiographic bone fill is also seen. The results have been maintained for 2 years.
*Reference: Constantinides C, Chang J, Fletcher P. Management of an Ailing Anterior Implant Utilizing a Minimally Invasive Flapless Surgical Technique: A Case Report. Clinical Advances in Periodontics. 2017 Oct 16(0):1-3.
{kind=link}
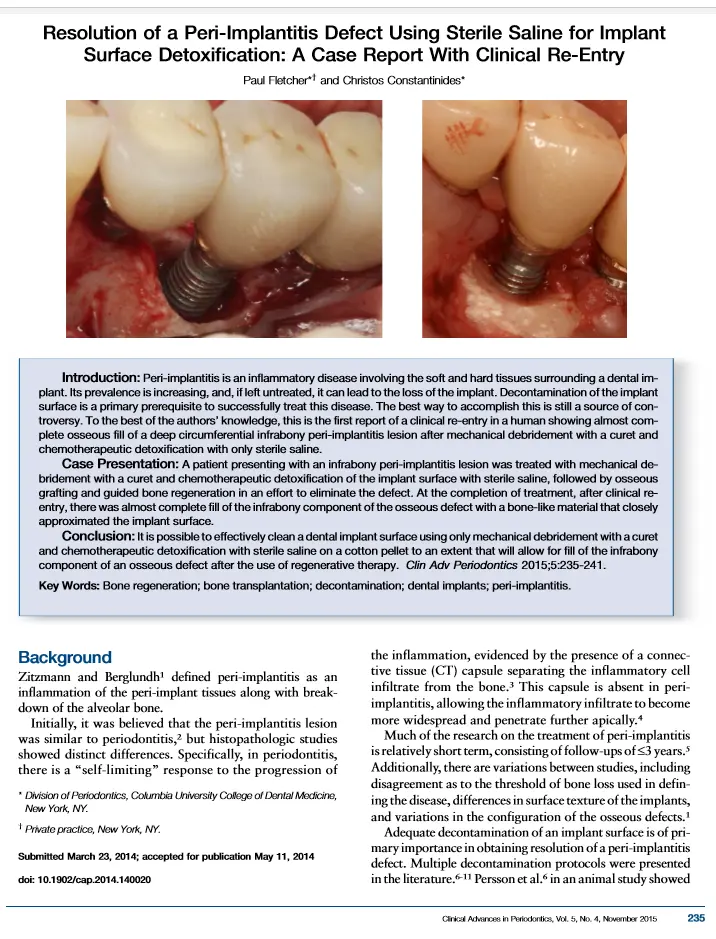
Resolution of a peri-implantitis defect using sterile saline for implant surface detoxification: A case report with clinical re-entry
Peri-implantitis is an inflammatory disease involving the soft and hard tissues surrounding a dental implant. Its prevalence is increasing, and, if left untreated, it can lead to the loss of the implant. Decontamination of the implant surface is a primary prerequisite to successfully treat this disease. The best way to accomplish this is still a source of controversy. To the best of the authors’ knowledge, this is the first report of a clinical re-entry in a human showing almost complete osseous fill of a deep circumferential infrabony peri-implantitis lesion after mechanical debridement with a curet and chemotherapeutic detoxification with only sterile saline.
*Reference: Fletcher P, Constantinides C. Resolution of a peri-implantitis defect using sterile saline for implant surface detoxification: a case report with clinical re-entry. Clinical Advances in Periodontics. 2015 Nov;5(4):235-41


Frequently Asked Questions
We will be as gentle as possible. The periodontal exam can be completed with little or no discomfort.
We will need current periodontal x-rays in order to see disease not otherwise visible. If your referring dentist has taken x-rays, you may request that they be forwarded to us.
Since all patients are different, your periodontist must complete your examination before establishing your treatment planning and the fee for care. The fee for periodontal treatment can vary considerably depending on the type of problems and the complexity and length of treatment. An approximate fee can usually be determined at the initial visit; but on occasion, some initial treatment or further diagnostics must be completed before the final treatment planning can be established. Our philosophy of practice is to treat as conservatively as possible to attain treatment goals.
Dental insurance policies often cover periodontal treatment. Please bring all medical and dental benefit information and cards to your examination appointment.
Not everyone needs periodontal surgery. If treated early, gum disease can be controlled without surgery. We will make recommendations based on your individual situation. Our philosophy of practice is to treat as conservatively as possible to attain treatment goals.
The recent advances in periodontal treatment allow us to successfully treat most teeth.
Our office and your dentist will work closely together. If crowns and fillings are needed your dentist will provide them. Regular visits to your dentist are an important part of periodontal maintenance.
Periodontal disease is a progressive, painless infection. Delay can cause you further bone loss and more expense. If your teeth are lost, dentures are never as effective as your own natural teeth.
After tooth extraction, if the walls of the socket are very thick, they will usually fill naturally with bone in two to three months. However, when the walls of your socket are very thin (such as in your upper and lower front teeth), this type of healing will not be as predictable. In these situations, a bone graft is often placed at the time of tooth extraction to help your body fill in the empty socket with bone. This step will maintain the width and volume of bone you will need for implant placement several months later.